
In the acute care setting, or any setting where they are present, lines, leads, tubes and drains can be the most intimidating aspect- especially as a student or new practitioner. During my 12-week rotation in acute care, I got to experience almost every kind of line, lead, tube or drain attached to a patient, and thus developed some skills and tricks to managing them effectively to ensure the safety of my patients. So without further ado, here are my tips and tricks to managing those pesky lines and leads!
1. Ask the nurse!
Before seeing any patient it is always important to talk to their nurse. The nurse knows everything about the patient and can give you a heads up on important information, precautions, and may even detach any lines or leads during treatment so that there is one less thing to worry about.
2. Take it SLOW
Before you even think about getting a patient up out of bed, or even sitting up in bed, take your time to visually scan the room, around the bed, and the patient to get a feel for the lines and leads that they may have attached. If there is a monitor on in their room reporting heart rate, oxygen saturation, respiratory rate and blood pressure, then you can already guarantee that they have multiple leads on their body.
As you are talking to the client and introducing yourself (and once you’ve gotten consent to treat/evaluate), make a point to walk around the bed to visually scan the area. Many devices, bags, and tubes may be under the bed, hanging from the bed or beside the bed.
And lastly, before you instruct the patient to get up, ask if you can remove their covers, and then visually inspect their body and make note of IVs, chest tubes, drains, restraints or any other lines attached. Take this time to not only make note of everything, but detangle lines, ensure that nothing is leaking, and notify the patient of any precautions and that movement may be restricted. The patient needs to take it slow too!
3. Know the precautions
As with any condition or injury, it is incredibly important to know precautions for specific lines, drains, tubes and leads. If a mistake is made a lot of problems can happen, from blood getting everywhere (it’s pretty gross), to compromising a life-saving surgery. Before entering a patient’s room, understand what their precautions are, verbalize the precautions and make sure that the patient understands them, and when in doubt – ASK THE NURSE!
Common Lines, Leads, Drains, and Tubes and Their Precautions
EKG
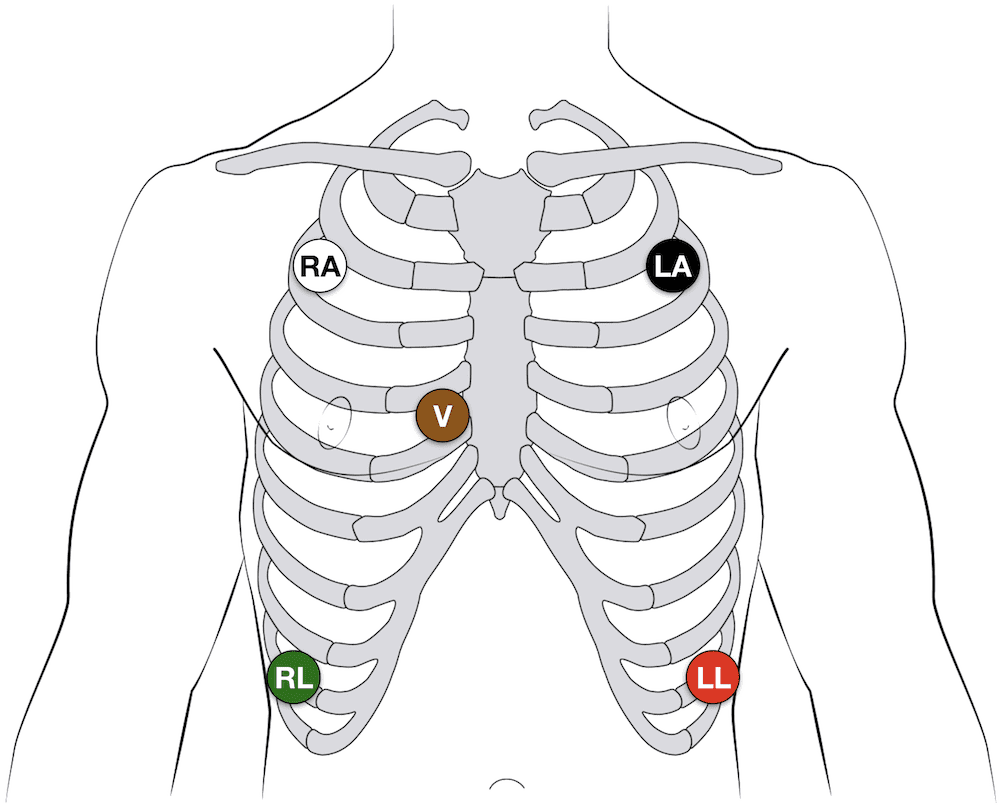
Telemetry Leads are placed on the client’s torso and can include anywhere from 3-12 leads. The most common placements you’ll see are like the picture to the left, with 5 leads. These leads are placed specifically so as to measure heart muscle contraction and rate.
Be aware of the presence of these leads and avoid pulling on them, getting them wet, or taking them off.
Make note of the type of device the leads are attached to, it will either be the main monitor attached to the wall (limiting movement), or a portable device that can be placed in the client’s gown pocket.
If a lead falls off during a session make sure to place it exactly on the spot it fell from, if you didn’t see where it fell from and you aren’t sure of where to place it, notify the nurse.
If the pad has lost its stickiness, you will need to notify the nurse so that they can bring in fresh pads.
Oxygen

A Nasal Cannula will be one of the most common tubes you will see in acute care.
Make sure to note the amount of oxygen the client is receiving, it will be measured in liters per minute.
If you are seeing the patient in their room, they will most likely be connected to the oxygen supply via a wall outlet- make note of the length of the tubing. If there is sufficient tubing the patient may be able to stand and walk around the room.
If there is insufficient tubing or you plan to leave the room for treatment, you will need to acquire a portable oxygen tank. Make sure to note the available oxygen in the tank, and when hooking up the patient’s oxygen tube, make sure to set the oxygen release rate to the amount prescribed for the patient.
You are NOT allowed to change the liter/minute without consulting the prescribing doctor.
Photo from Science Photo Library / Getty Images

BiPAP and CPAP
For patients with difficulty regulating their breathing cycles (such as with sleep apnea), they will require either BiPAP or CPAP, and it may look something like in the picture.
BiPAP provides an inhalation pressure and an exhalation pressure, while CPAP only applies a single pressure to regulate normal breathing patterns.
These machines may make grooming ADLs difficult as the mask is required to stay on (unless the doctor allows for use of a nasal cannula during waking hours).
Out of bed activities may not be possible, so working with the patient while in bed may be necessary. Ensure that the mask’s seal remains tight throughout the session.
Photo: James Heilman, MD, 2014

Although tracheostomies are most often going to be seen in the ICU or stepdown units, it is possible to see them in any setting, especially for those who are dependent on ventilators for breathing (i.e. high-level spinal cord injury).
It can be very intimidating to work with a client who has a tracheostomy, but as long as you are careful to avoid pulling or snagging any tubing, full range of motion and participation in activities is possible.
It is also important to remember that the presence of a tracheostomy means that the patient will be unable to speak, as any expelled air is released through the trach and therefore does not pass through the vocal cords. So give them time to respond to your questions, or if they prefer, allow them to write on a white board or paper.
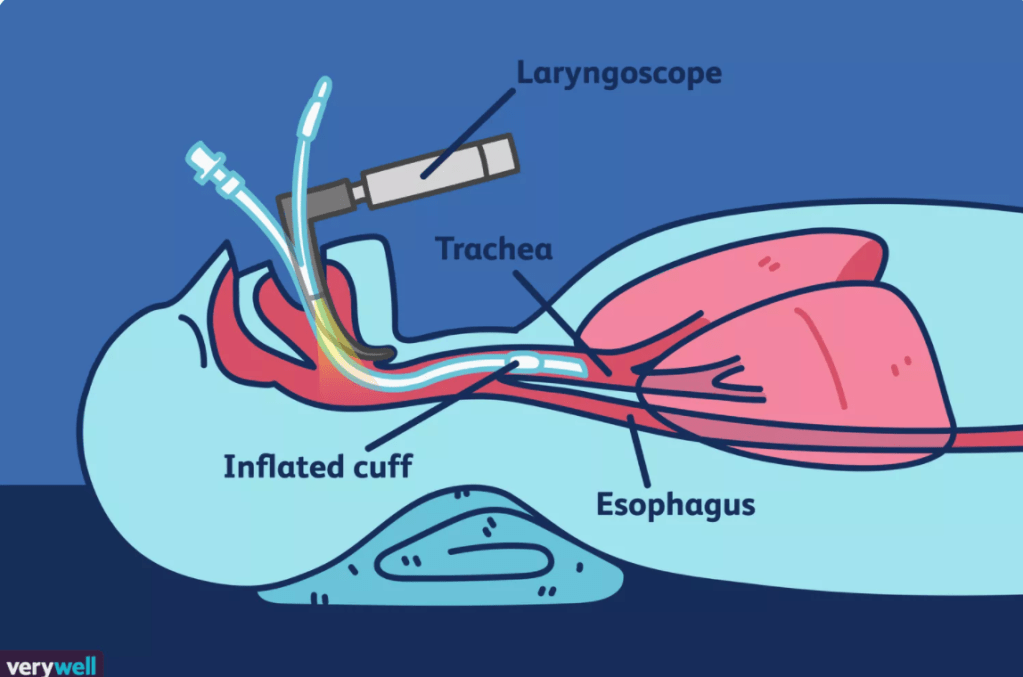
Endotrachial intubation will most often be seen in the ICU, and similar to a tracheostomy, the patient will be hooked up to a ventilator. However, unlike a tracheostomy, the tubing will go directly into the patient’s mouth and down their airway to reach right above the lungs.
While the patient will be most likely unconscious or sedated if they are intubated, it is also possible that they will be able to respond to simple commands or open their eyes.
Just as with the tracheostomy, you will want to avoid awkward positions of the tubing (which may initiate a gag reflex or cause discomfort), tugging or pulling on the tube, and if the patient is able to move their upper extremities make sure that they are not able to pull on the tubes themselves.
Illustration by Joshua Seong. © Verywell, 2017.

Pulse oximetry is used to measure the amount of oxygen in one’s blood, and is measured with a small device, like the one pictured. Other devices may include a flat sticky pad that can be placed on the finger or even the forehead. It is also possible that a clip will be placed on the earlobe to measure the oxygen saturation.
It is very important to keep the reader attached if the patient’s diagnosis involves poor oxygen saturation levels and monitoring of their oxygen is important during tasks and physical exertion.
Image from: https://www.healthline.com/health/pulse-oximetry#purpose-and-uses
Catheterization
External Catheter – Purewick or Condom Catheter

These catheters are placed externally on the patient (i.e. if it falls off, the patient won’t start bleeding, but they may start urinating unknowingly). A ‘Purewick’ is an external catheter for females, and is usually attached to suction via a long tube. Since it is attached to suction, it is important to make note of the length of the tubing when planning for out of bed activities. If the tubing is not long enough, you can detach the tube, unless fluid measurement is important, then ask the nurse.
Image from: https://www.purewickathome.com/purewick-how-it-works/
Similarly, a condom catheter sounds exactly like you think. And these things… fall off a lot. Don’t panic if this happens though, if it falls off do not try to put it back on, just notify the nurse! If there are briefs available in the room it would be a good idea to put them on, chances are, if the patient has a catheter on/in, then they can’t tell when they have the urge to go.
A Foley Catheter is the type of catheter you are probably familiar with. This type of catheter goes straight up the urethra to the bladder, and a small balloon is inflated once inside the bladder to prevent the tubing from slipping out. This means – DO NOT TUG IT. I had a patient pull out 3 foley catheters (before I worked with him), and the amount of blood that comes out is way too much.

These catheters will drain into a portable bag that is most often clipped to the side of the bed. So, before you start bed mobility and getting out of bed, make sure to move this bag so as to avoid any pulling or tugging. If we got up and walked I would clip the bag to my scrub pants (keeping it below the level of the patient’s bladder – very important!), but if they use a walker to ambulate, you can clip the bag onto the walker. It is also important to keep the collection bag from touching the ground – for sanitary reasons.
Image from: https://www.jaga-me.com/caregivers-guide-urinary-catheter/
A Suprapubic Catheter is surgically inserted into the bladder through a small incision in the lower abdomen. This type of catheter is generally more comfortable than a foley catheter because it doesn’t have to go through the sensitive tissue of the urethra, but it is also important not to snag the tubing. The catheter tubing may drain into a bag or may have a valve at the end to allow for controlled draining.
Someone who has a suprapubic catheter will likely have it long-term or permanently. Common reasons to have a suprapubic catheter are because of health conditions such as a spinal cord injury that prevent the individual from having voluntary control of urination, or trauma to the urethra.
A very important thing to keep note of when working with someone who uses a catheter is this: do NOT hold the bag above the waist, if you do, urine may travel back into the bladder and this could lead to a bladder infection. It is also important to avoid kinking the tubing, do not let the patient sit or lay on the tubing as this can kink the tube and cause urine to backflow.
Intravenous
Intravenous Catheter, we all pretty much know what an IV is. Common placements include wrist, elbow and neck, and it is always very important to make note of two things: the length of the IV tubing, and the appearance of the IV site. If the area around the IV placement is red, swollen, bleeding, leaking, and/or painful, it is important to notify the nurse. The length of the tubing will tell you how much movement the patient is allowed to do, but if you have a portable IV pole, you will be able to transfer the bag and infusion pump so that your patient can stand up and ambulate.

Central Venous Catheter, also known as a central line, is inserted just below the collarbone (clavicle), into a large vein in the neck. Just as with all of lines and tubes, be sure not to touch the placement site, if you notice the tape holding the lines has come unstuck, notify the nurse so that they can fix it. Do not get the placement site wet, and of course, do NOT tug! Limit upper extremity movement on the side of the central line placement as this may cause unnecessary discomfort for the patient.
Image from: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/central-venous-access-catheter

PICC Lines are inserted in to the upper arm and may have extra tubes hanging off of the placement site. Avoid applying pressure to this site or of course, tugging the lines.
Image from: https://infusionsolutionsinc.com/what-is-a-picc-line

A Port is about the size of a quarter and is surgically implanted under the skin. You will commonly see a lump under the collarbone, usually on the right side. This device is used by doctors to administer medications and draw blood, and is kept under the skin long-term. The only precautions are during the healing process and when there is a needle in the port. If the port is new and there is still an unhealed wound where it was placed, do not allow the patient to lift over 10 pounds or participate in any heavy activities that could prevent it from healing. Once it has completely healed, the patient will be able to live life as normal. Just keep an eye out for any swelling or redness around the port placement.
Image from: https://nurse.org/articles/what-is-a-port-a-cath/
Peripheral Arterial Lines
Arterial Lines, or Art-Lines, are placed in the wrist and are used to measure blood pressure and draw blood. It is important to avoid movement or activity where the line is placed, as this may cause twisting or cinching of the line. Often, the patient will have a splint that prevents them from moving the body part where the art-line is placed – ensure that they comply with this precaution, and do not take range-of-motion at this joint.
Feeding Tubes

Naso-Gastric Tube (NG Tube) and Oral-Gastric Tube (OG Tube), these tubes are placed either into the nose or mouth, respectively, and extend into the stomach. You may think that these tubes only supply nutrition to the patient, but they can also be hooked up to a suction device that empties the stomach of its contents. Whatever it is being used for, you do not want to tug on these tubes, and avoid moving them too much as this may cause a lot of discomfort for your patient. These tubes are often held in place with tape on the nose, if you notice the tape is coming unstuck, notify the nurse so that they can reapply tape.
G-Tubes and PEG Tubes are similar to NG/OG Tubes in that they provide nutrition, however they are placed directly into the stomach via a small incision in the abdomen. This type of tube is less likely to be tugged and allows the patient to have their face free. ADLs such as face-washing, teeth brushing and hair-washing will be easier to complete since they do not have a sensitive tube on their face.
Drains
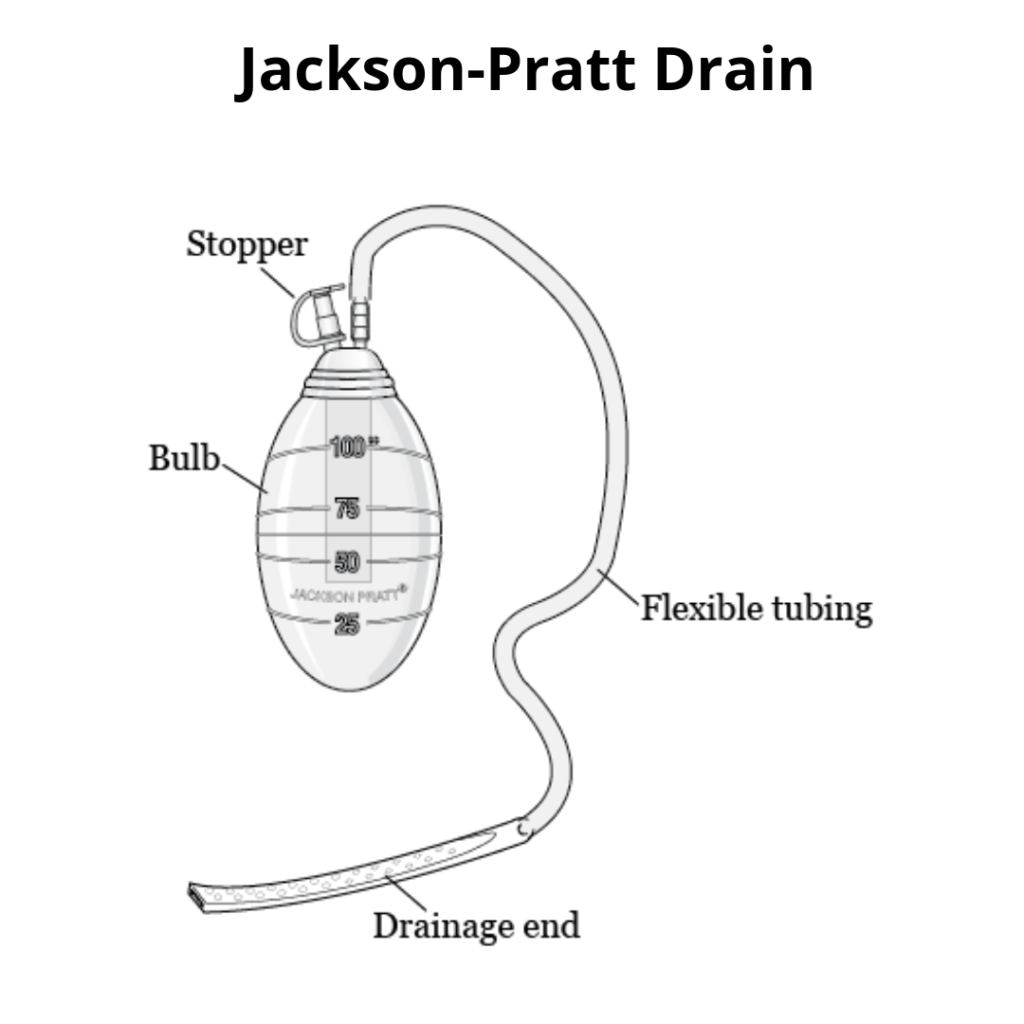
A Jackson-Pratt Drain (JP Drain) is a small, flexible bulb-like drain that is placed after a surgery and is held in place by sutures. This little bulb will hang from the surgery site so it is very important not to tug on this, and when possible, place it in the patient’s gown pocket or strap is somewhere where it won’t hang freely and get caught on anything. Observe for any redness or swelling around the placement site.
Image from: https://www.saintjohnscancer.org/melanoma/patient-resources/jackson-pratt-jp-drain/

Chest Tubes (thoracic catheter, tube thoracostomy, intercostal drain) are placed between two ribs and are used to drain fluid, blood or air that is trapped between the ribs and lung. The collection box is usually placed on the floor next to the bed and it is important to keep this box upright so that accurate measurement of the drained contents can be attained. Chest tubes can often be very painful for the patient, especially with upper extremity movement. So while it is important to conduct the therapy session, you may want to be considerate when asking the patient to do overhead activities or if they state that a certain movement causes a considerable amount of pain.
Image from: https://thoracics.org/2015/08/24/developments-in-chest-tube-management/
Neuro
An Intracranial Pressure Monitor (ICP Monitor), is surgically placed beneath the skull and is used to read the pressure around the brain. If your patient has this monitor, it is extremely important to monitor their ICP throughout the session to avoid increasing pressure. The pressure range is determined by the doctor and should always be confirmed with the nurse before proceeding with therapy. If you notice their ICP is increasing, stop the activity immediately and notify the nurse.

A Ventriculostomy is an extremely sensitive piece of equipment. This is a type of catheter that is inserted into the ventricles of the brain, yeah, IN the brain. This device is used to measure and control the pressure in the brain, and the most important part about it, is that the head of the bed must remain at a very specific height and the collection system is measured so precisely, that they actually use a level. Do not start treating these patients without confirmation from the nurse!
Other
Wound Vacs are placed to aid in the wound healing process. These are usually used for larger wounds that need extra help to close. This is done by tightly sealing the area and applying negative pressure through a wound vac pump. It is very important to keep that seal tight, so d avoid any tugging of the tubing and getting the seal wet. (I won’t include an image, they’re not very pretty.)
Though it can be intimidating, and it may take some time to become comfortable working around these lines and tubes, remember that it is still important to get the patient up and to continue with therapy (as long as you are safe!) Early mobility is very important in the acute setting, and if you are afraid of moving the patient on your own, simply ask someone to help you – whether that is a nurse, an aid, or a fellow therapist that may have some extra time.

Great post very informative.
LikeLiked by 1 person
As a student in their acute care rotation, this was super helpful!
LikeLike
Thank you so much. I am trying to review these concepts in preparation for my advanced competency next week, and I’m going to bookmark this page to also revisit before I start my acute care rotation this Spring. It really helped to read about these lines and drains from an OT’s perspective, and your pictures and summaries were perfect!
LikeLike
This is such a comprehensive article. Great for new grad nurses or the family caregiver. I just like to add that my mom who is a nurse invented a product to organize medical lines and keep them off the floor! I am spreading the word about it to help with patient safety. It’s called The Beata Clasp.
LikeLike